https://zenblis.com/glossary/polst
POLST (Portable Medical Orders)
A POLST translates a seriously ill patient's wishes for end-of-life care into a portable medical order that paramedics, hospitals, and nursing homes are legally required to follow. Different from an Advance Directive — and often more operationally consequential.
By Derek Belfield - 2026-04-27
Definition
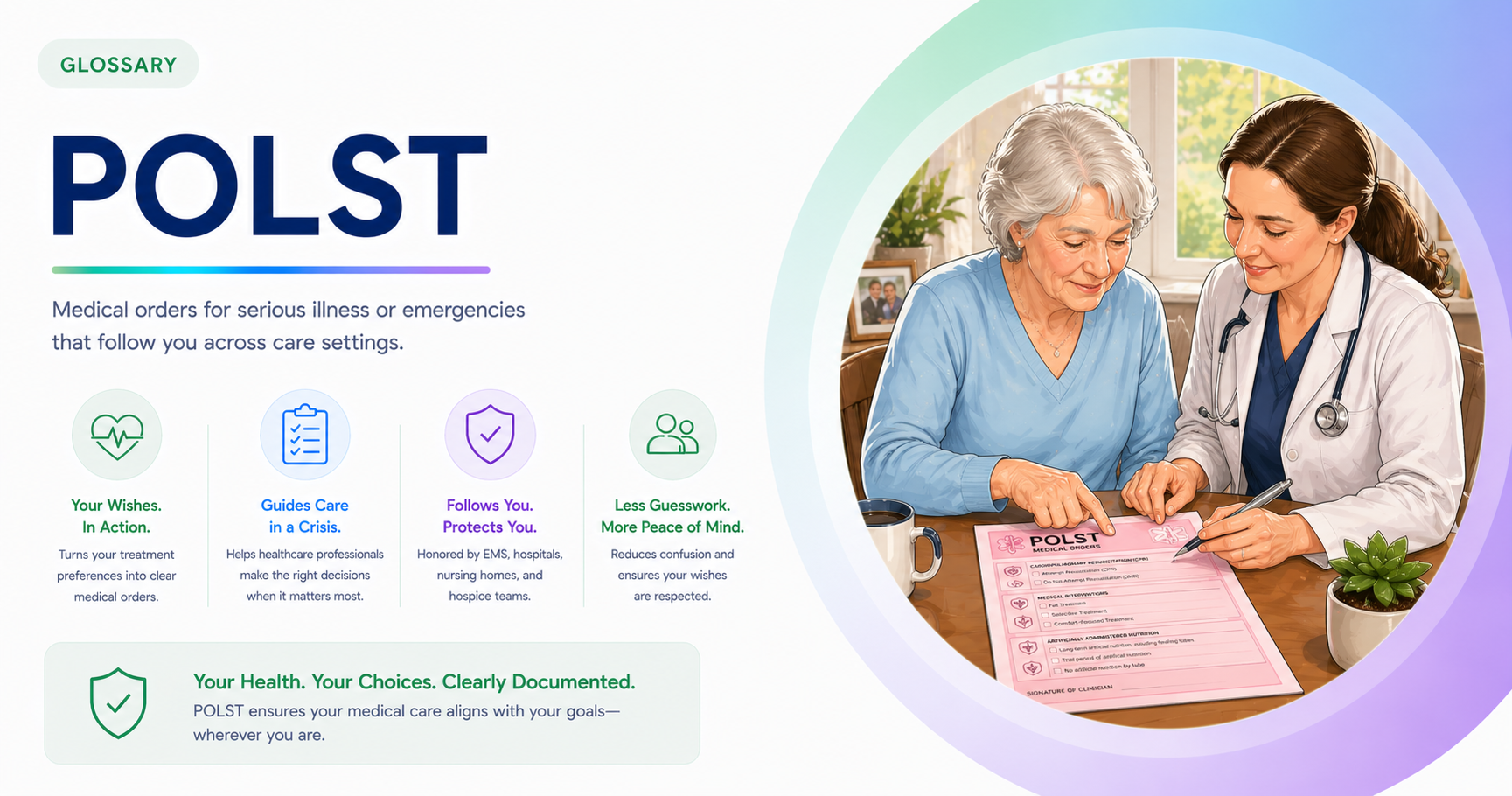
A POLST — Portable Medical Order, also called Physician Orders for Life-Sustaining Treatment — is a brightly colored, single-page medical order signed by both a clinician and a seriously ill patient that translates the patient's wishes for end-of-life care into immediately actionable instructions any healthcare provider must honor, including emergency responders and across care settings.
Expanded definition
A POLST is the document that bridges the gap between an Advance Directive — which is a legal expression of preferences — and the actual medical decisions made in an emergency. The distinction matters more than most families realize. When a 911 call is made and emergency responders arrive, they are legally required to provide full life-saving interventions by default, including CPR, intubation, and aggressive resuscitation, unless they see a valid medical order telling them otherwise. An Advance Directive alone does not stop them. A POLST does. This is why for a seriously ill or frail patient, the POLST is often the most operationally consequential document they will ever sign.
History of the POLST
The POLST began in Oregon in 1991, when a state task force recognized that Living Wills and Advance Directives, however well-intentioned, were rarely available or honored at the moment when emergency decisions had to be made. Oregon developed a portable medical order — a brightly colored, standardized form designed to travel with the patient across hospitals, nursing homes, hospice, ambulances, and home. The form was first used in 1995 and has since been adopted in 46 states under various names. Different states call it POLST (most states), MOLST (New York, Massachusetts, Maryland, and several others), POST (West Virginia, Tennessee), MOST (North Carolina, Colorado), COLST (Vermont), and TPOPP (Kansas, Missouri). The names vary; the function is consistent.
Difference between a POLST and an Advance Directive
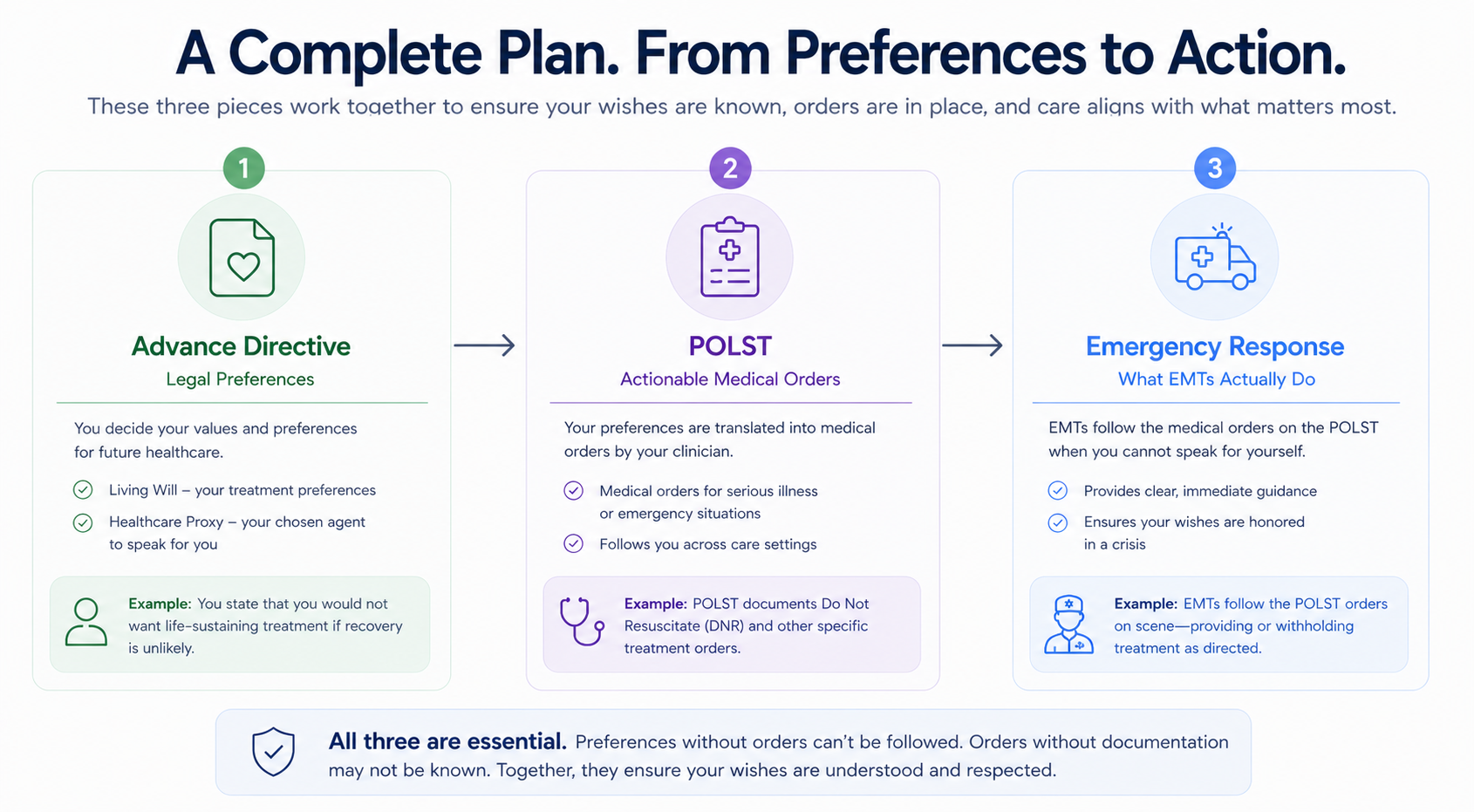
A POLST is fundamentally different from an Advance Directive in three ways:
First, a POLST is a medical order, signed by a clinician — usually a physician, nurse practitioner, or physician assistant depending on the state — which means healthcare providers including paramedics and EMTs are legally required to follow it. An Advance Directive is a legal document expressing wishes; a POLST is an actionable order.
Second, a POLST is intended only for patients who are seriously ill or frail near the end of life, while an Advance Directive is appropriate for any adult. The "surprise question" clinicians often use as a guide: if the clinician would not be surprised if this patient died within the next year, the patient is probably appropriate for a POLST.
Third, the POLST is portable — it must be honored across all care settings, including in the patient's own home if EMS responds to a call there.
What an Advance Directive looks like
The form itself is short — typically a single page on bright pink, green, or yellow paper, designed to be visually impossible to miss in a medical record or on a refrigerator. Most state versions cover four sections: cardiopulmonary resuscitation (CPR yes or no if the patient has no pulse and is not breathing), medical interventions (the level of treatment if the patient has a pulse but is critically ill — comfort measures only, limited additional interventions, or full treatment), antibiotics (yes, no, or trial period for life-threatening infections), and artificial nutrition and hydration (yes, no, or trial period). The form is signed by both the clinician and the patient (or the patient's healthcare agent if the patient lacks capacity), reviewed regularly as the patient's condition changes, and travels physically with the patient between care settings.
The bottom line
For senior care families, a few practical realities matter. A POLST is voluntary; no one can be required to complete one as a condition of admission to any facility. It is not a substitute for a Healthcare Power of Attorney or Living Will — most patients with a POLST also have an Advance Directive, and the two work together. The POLST should be visible: on the front of the medical chart in a facility, on the refrigerator at home where EMS will see it, and a copy with the named healthcare agent. Most state POLST programs maintain registries that allow electronic access by emergency responders. A POLST can be revoked or revised at any time — by the patient if competent, or by the healthcare agent following the patient's known wishes — by signing a new form that supersedes the prior one. And finally, families should know that a POLST is not a permanent decision. As a patient's condition changes, so should their POLST, which is why most states require periodic review with the signing clinician.
Frequently Asked Questions
- What's the difference between a POLST and an Advance Directive?
- An Advance Directive is a legal document expressing your medical wishes; a POLST is a medical order signed by a clinician that healthcare providers are legally required to follow. An Advance Directive is appropriate for any adult and covers many possible future scenarios. A POLST is intended only for seriously ill or frail patients near the end of life, and translates their wishes into specific, actionable orders that paramedics, hospitals, and nursing homes must honor immediately — including in emergencies. Most patients with a POLST also have an Advance Directive; the two work together.
- Why is a POLST printed on brightly colored paper?
- The bright color — typically pink, green, or yellow depending on the state — is intentional. POLST forms are designed to be visually impossible to miss in a medical chart or on a refrigerator door, so emergency responders, hospital staff, and nursing home caregivers can spot them quickly. In a medical emergency, the form needs to be found and read in seconds. The color choice is part of why the document works as a portable medical order rather than just another piece of paperwork.
- Who is a POLST appropriate for?
- A POLST is appropriate for patients who are seriously ill or frail near the end of life — typically those whose physician would not be surprised if they died within the next year. This includes patients with advanced cancer, end-stage heart failure, advanced COPD, advanced dementia, late-stage Parkinson's disease, ALS, or significant frailty in late old age. A POLST is not appropriate for healthy adults, who should instead have an Advance Directive. The form is voluntary; no patient is required to complete one as a condition of admission to any care setting.
- What does a POLST form include?
- Most state POLST forms include four sections. Section A covers cardiopulmonary resuscitation (CPR or no CPR if the patient has no pulse and is not breathing). Section B covers medical interventions if the patient has a pulse but is critically ill — comfort measures only, limited additional interventions including IV fluids and cardiac monitoring, or full treatment including intubation and intensive care. Section C covers antibiotics for life-threatening infections. Section D covers artificial nutrition and hydration through feeding tubes or IV. The form is signed by both the clinician and the patient or the patient's healthcare agent.
- Will my POLST be honored in a different state?
- Most states honor a POLST executed in another state, but state-specific forms are usually preferred because they remove ambiguity for local emergency responders and hospitals. The form names also vary — POLST in most states, MOLST in New York and Massachusetts, MOST in North Carolina, POST in West Virginia, COLST in Vermont, TPOPP in Kansas and Missouri. For seniors who split time between states, asking the local physician about that state's specific portable medical order is the standard recommendation.
- Is a POLST the same as a DNR?
- No, but they overlap. A DNR — Do Not Resuscitate — is a specific medical order that says no CPR if the patient's heart or breathing stops. A POLST is a broader portable medical order that includes the CPR decision in Section A but also addresses medical interventions, antibiotics, and artificial nutrition. A POLST can include a DNR order as part of its content, but it covers significantly more ground. Some patients have only a DNR; others have a POLST that includes a DNR plus other orders; some have both as separate documents.
- Can a POLST be changed after it's signed?
- Yes. A POLST should be reviewed periodically as the patient's condition or wishes change, and updated by signing a new form that supersedes the prior one. The patient can revoke or revise the POLST at any time while they have decision-making capacity. If the patient lacks capacity, the named healthcare agent can request changes following the patient's known wishes. Most state POLST programs require review at least annually for patients in nursing homes, when the patient transfers between care settings, when the patient's condition substantially changes, or when treatment preferences change.