https://zenblis.com/glossary/rehabilitation
Rehabilitation
Post-acute rehabilitation happens in either an Inpatient Rehabilitation Facility (intensive, hospital-level) or a Skilled Nursing Facility (less intensive, longer stay). The setting choice shapes recovery outcomes and Medicare costs.
By Derek Belfield - 2026-04-26

Definition
Rehabilitation in senior care refers to short-term, medically necessary therapy — physical, occupational, or speech — that helps a person recover function after a hospitalization, surgery, stroke, or major medical event, delivered either in an Inpatient Rehabilitation Facility (IRF) or as part of a stay at a Skilled Nursing Facility (SNF).
Expanded definition
Rehabilitation in senior care almost always means post-acute rehabilitation: a recovery period following a hospital stay where the goal is to regain physical, occupational, or cognitive function before returning home. The most common rehab triggers are stroke, hip fracture, joint replacement, traumatic brain injury, cardiac events, and major surgery. Therapy disciplines involved typically include physical therapy (PT), occupational therapy (OT), and speech-language pathology (SLP), often delivered together as a coordinated plan of care.
Rehab settings
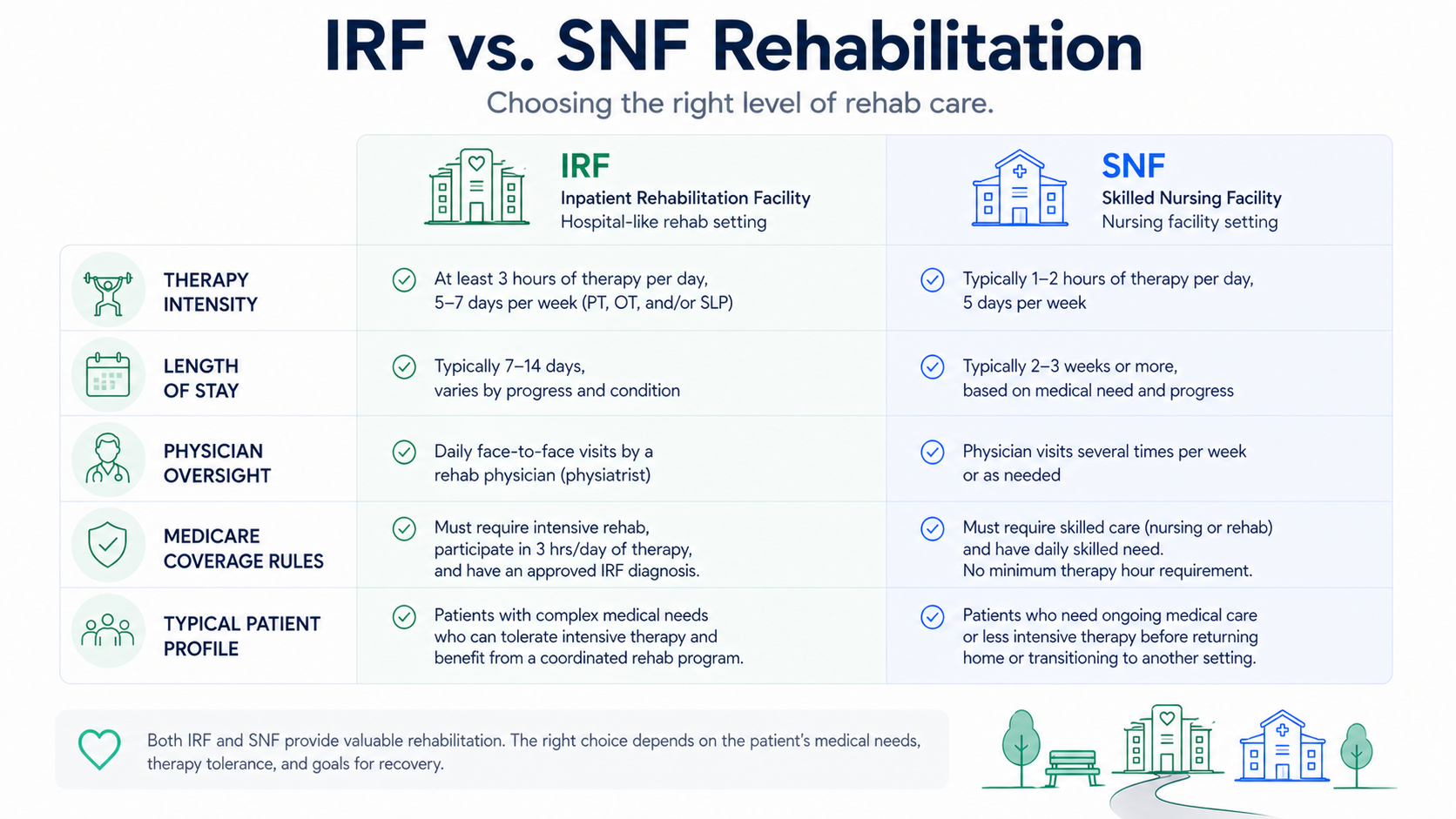
Two settings provide post-acute rehabilitation, and the choice between them shapes both the recovery trajectory and the family's financial exposure. Inpatient Rehabilitation Facilities (IRFs) are licensed as hospitals, staffed with rehabilitation physicians who see patients at least three times a week, and required by Medicare to provide intensive therapy — at least three hours per day, five days a week. Average IRF length of stay is roughly 10 to 14 days. Skilled Nursing Facilities (SNFs) provide what is sometimes called sub-acute rehabilitation: less intensive therapy, often 1 to 2 hours per day, with a physician required to see the patient only every 30 days. Average SNF length of stay for rehabilitation is longer than at an IRF, typically 20 to 30 days. Research consistently shows that for stroke and hip fracture patients, IRFs produce better outcomes than SNFs for similar diagnoses — but only patients who can tolerate the intensive schedule are candidates.
Medicare coverage
Medicare coverage rules differ between the two settings in ways families should understand before discharge. IRFs are covered under Medicare Part A as hospital care, with no qualifying three-day inpatient stay required and a benefit period structure that pays the first 60 days in full after the deductible. SNF rehabilitation requires a qualifying three-day hospital inpatient stay (observation status does not count), covers the first 20 days in full, then charges a daily copay through day 100. The hospital discharge planner typically recommends the appropriate setting based on the patient's medical complexity, therapy tolerance, and functional baseline — but families have the legal right to choose.
Other forms of "rehab"
Beyond post-acute rehab, the term is sometimes used more broadly. Outpatient rehabilitation refers to therapy a patient receives in a clinic without an overnight stay, often after IRF or SNF discharge. Long-term acute care hospitals (LTACHs) provide complex medical care to patients who need extended hospital-level treatment along with rehabilitation. Some assisted living and CCRC communities also offer therapy services to residents under Medicare's outpatient benefit. Throughout the senior care system, families should always ask which specific Medicare benefit is being used, because the coverage rules and financial exposure differ significantly across these settings.
Frequently Asked Questions
- What's the difference between an IRF and SNF rehabilitation?
- An Inpatient Rehabilitation Facility (IRF) is a hospital-licensed setting providing intensive therapy — at least three hours per day, five days a week — with rehabilitation physicians on-site three times a week. A Skilled Nursing Facility (SNF) provides less intensive therapy, often 1 to 2 hours per day, with physicians required to see patients every 30 days. IRFs typically have shorter stays (10–14 days) and better outcomes for patients who can tolerate intensive therapy; SNFs are appropriate for patients who need rehabilitation but can't tolerate the IRF pace.
- Does Medicare cover rehabilitation?
- Yes, but the rules differ by setting. IRF stays are covered under Medicare Part A as hospital care, with no qualifying three-day hospital stay required and the first 60 days fully covered after the deductible. SNF rehabilitation requires a qualifying three-day inpatient hospital stay (observation status doesn't count), covers the first 20 days in full, and charges a daily copay through day 100. Outpatient rehabilitation is covered under Medicare Part B with standard cost-sharing.
- How is the rehabilitation setting decided?
- The hospital discharge planner typically recommends the setting based on the patient's medical complexity, therapy tolerance, and functional baseline. Patients who can tolerate three or more hours of therapy per day and have rehabilitation potential are typically referred to an IRF. Patients who need rehabilitation but can't tolerate the IRF pace, or who need ongoing medical supervision, are typically referred to a SNF. Families have the legal right to choose any Medicare-certified facility with an available bed.
- Why do IRFs tend to produce better outcomes than SNFs?
- Research published in the American Journal of Managed Care and other peer-reviewed journals has found that for stroke and hip fracture patients, IRFs are associated with lower mortality, more days at home, fewer emergency room visits, and faster functional recovery compared with SNFs. The likely drivers are higher therapy intensity (about 17.5 hours per week at an IRF vs. 8.9 hours per week at a SNF, in stroke comparisons), more frequent physician oversight, and 24-hour registered nursing staff. Patient selection matters — only patients who can tolerate intensive therapy are IRF candidates.
- What's sub-acute rehabilitation?
- Sub-acute rehabilitation is the term for the rehabilitation services provided in a Skilled Nursing Facility (SNF). It refers to the lower intensity of therapy compared with the acute, hospital-level rehabilitation provided in an Inpatient Rehabilitation Facility (IRF). Patients in sub-acute rehab typically receive 1 to 2 hours of therapy per day across PT, OT, and speech-language pathology, depending on tolerance and physician orders.
- What happens when rehabilitation ends?
- Most rehabilitation patients return home, sometimes with a referral for outpatient therapy or Medicare home health services to continue recovery. Some patients transition from an IRF to a SNF for continued recovery at lower intensity before going home. A subset of rehabilitation patients — often those who don't recover sufficient function — transition from short-term rehabilitation to long-term nursing home care, with payment shifting from Medicare to private pay or Medicaid.